Every podiatrist knows the sting of a denied claim. What most don’t realize is how often Q7, Q8, and Q9 are behind it. These tiny modifiers might look harmless, but misuse them once and you’re staring at weeks of lost revenue. This isn’t about “just knowing the codes.” It’s about protecting your practice from silent revenue leaks hiding inside routine foot care billing.
Confusion ends here. Inside, you’ll find a clear breakdown of what each modifier means, along with the clinical logic behind it. So you can code with confidence every time.
When & Why Q Modifiers Turn Routine Foot Care into Billable and Covered Services?
Medicare has one clear starting point: routine foot care isn’t covered. The only time it is covered is when your patient has a qualifying condition, when it would be unsafe for anyone other than a professional to provide that care, and when your notes line up with the rules written in your local LCD.
Those LCDs are basically the checklists your regional Medicare office uses to decide if a claim should be paid. Q7, Q8, and Q9 are the keys that show you’ve met those rules. Used correctly, they make your claim clear and defensible. Used loosely, they almost guarantee a denial.
What Q7, Q8, and Q9 really mean?
Q modifiers are a shorthand that tells Medicare which specific risk findings you saw in the same foot on the date of service. They exist to turn routine foot care into payable care when risk is real and documented.
The core definitions
1- Q7 Modifier
One Class A finding. In practice, this means a nontraumatic amputation of the foot or an integral skeletal portion of the foot. Document level and laterality, for example, transmetatarsal amputation of the left foot.
2- Q8 Modifier
Two Class B findings in the same foot. Class B includes either absent dorsalis pedis pulse, absent posterior tibial pulse, or advanced trophic changes. Advanced trophic changes count as a single Class B finding but must be proven by three specific skin or nail signs in the same foot.
3- Q9 Modifer
One Class B finding plus two Class C findings in the same foot. Class C includes claudication, temperature change such as cold feet, edema, paresthesias, and burning.
What counts inside each class?
Class A
Nontraumatic amputation of the foot or an integral skeletal portion of the foot. For example transmetatarsal amputation or amputation of a toe. Use Q7
Class B
Any of the following counts as one Class B finding per foot
a. Absent dorsalis pedis pulse
b. Absent posterior tibial pulse
c. Advanced trophic changes, which requires three findings in the same foot from this list
-
hair growth decrease or absence
-
nail thickening
-
pigmentary change or discoloration
-
thin shiny skin texture
-
persistent rubor or redness
Use Q8 when you have two Class B findings in the same foot. Examples that meet Q8
-
absent dorsalis pedis pulse plus absent posterior tibial pulse in the same foot
-
absent dorsalis pedis pulse plus advanced trophic changes proven by three skin or nail signs in the same foot.
Class C
-
Claudication
-
Temperature change such as cold feet
-
Edema
-
Paresthesias
-
Burning
Use Q9 when you have one Class B plus any two Class C in the same foot. Example that meets Q9
-
absent posterior tibial pulse plus edema and paresthesias in the same foot.
The per-foot rule
Apply and document class findings per foot. Do not mix left and right to reach a count. Your note should make it obvious which foot meets Q7, which meets Q8, or which meets Q9. Payers expect the modifier to reflect findings in the treated foot on that date of service.
When Q modifiers are expected on the claim
If you are seeking coverage for routine foot care based on a qualifying systemic condition, append one Q modifier to each affected line as appropriate. The CMS articles list the common codes where a Q modifier is required in this context which include 11055, 11056, 11057, 11719, G0127, 11720, and 11721.
The neuropathy exception
If the patient has peripheral neuropathy without vascular impairment and you are using the neuropathy exception, class finding modifiers are not required. Your documentation still must meet the LCD for that pathway
Documentation That Actually Defends the Modifier
-
Tie each finding to the same foot you treated. State left or right and specify toes when relevant.
-
For trophic changes, list three discrete signs rather than a generic phrase. For example thin shiny skin, nail thickening, persistent rubor documented in the right foot.
-
Link findings to the systemic condition that justifies coverage under your LCD, and include the active care requirement when your MAC marks a diagnosis with an asterisk. Many policies require proof that an MD or DO actively managed the complicating disease within the previous six months. Include name, NPI if required by the article, and last visit date.
Quick Practical Examples To Use Modifier Q7, Q8, Q9
Q7 example
Patient with a prior nontraumatic amputation of the right great toe presents for routine foot care. Note documents right great toe amputation with date and level. Routine foot care on the right foot reported with the appropriate CPT and Q7 on that line.
Q8 example
Left foot shows absent dorsalis pedis pulse and advanced trophic changes proven by thin shiny skin, nail thickening, and persistent rubor. Routine foot care for the left foot reported with the appropriate CPT and Q8 on that line.
Q9 example
Right foot shows absent posterior tibial pulse plus edema and paresthesias. Routine foot care for the right foot reported with the appropriate CPT and Q9 on that line.
Common pitfalls that trigger denials
-
Counting trophic changes without listing three specific signs.
-
Using a Q modifier for neuropathy without vascular impairment. The modifier is not required for that path.
-
Forgetting that the Q modifier is expected only when coverage is based on a qualifying systemic condition for the listed routine foot care codes.
Don’t Forget the Anatomy Modifiers
While Q modifiers explain why routine foot care is medically necessary, anatomy modifiers tell Medicare where the service was performed. Missing them is one of the most common and costly mistakes in podiatry billing.
Why They Matter
-
Q7, Q8, and Q9 show risk and medical necessity.
-
LT, RT, and T-modifiers show anatomical location.
-
Together, they create a complete picture that satisfies coverage rules.
-
Leave one out and the claim is flagged, denied, or delayed.
Foot Laterality Modifiers
-
LT → Left foot
-
RT → Right foot
Example:
11721 with Q8 + LT signals debridement of nails on the left foot with two Class B findings documented.
Toe-Specific Modifiers (TA–T9)
When treatment involves a toe, add the correct modifier to show exactly which digit was treated.

-
TA → Left great toe
-
T1 → Left second digit
-
T2 → Left third digit
-
T3 → Left fourth digit
-
T4 → Left fifth digit
-
T5 → Right great toe
-
T6 → Right second digit
-
T7 → Right third digit
-
T8 → Right fourth digit
-
T9 → Right fifth digit
Example:
11720 with Q9 + RT + T6 means: debridement of a nail on the right second toe, with one Class B and two Class C findings documented in the same foot.
Common Denial Triggers With Anatomy Modifiers
-
Reporting Q modifiers without specifying which foot was treated.
-
Forgetting to apply toe-level detail when only one or two digits are involved.
-
Using LT/RT inconsistently across multiple lines of service.
-
Applying toe modifiers without a corresponding Q modifier in cases where coverage hinges on systemic conditions.
|
Scenario |
CPT/HCPCS Code |
Q Modifier |
Anatomy Modifier |
Diagnosis Code(s) |
Explanation |
|
Patient with non-traumatic amputation of left great toe; routine nail care performed |
11719 (Trim nail(s)) |
Q7 (1 Class A finding) |
LT + TA (Left foot, left great toe) |
E11.51 (Diabetes with peripheral angiopathy) |
Q7 shows medical necessity (amputation history), LT/TA pinpoint location |
|
Patient with absent dorsalis pedis pulse + trophic changes in right foot; debridement of 6 nails |
11721 (Debride nails, 6+) |
Q8 (2 Class B findings) |
RT (Right foot) |
I70.203 (Atherosclerosis of extremities) |
Q8 proves risk (absent pulse + trophic changes), RT shows foot treated |
|
Patient with absent posterior tibial pulse + edema + paresthesias in left 2nd toe; nail debridement |
11720 (Debride nails, 1–5) |
Q9 (1 Class B + 2 Class C findings) |
LT + T1 (Left foot, 2nd toe) |
E11.42 (Diabetic polyneuropathy) |
Q9 ties findings together, LT/T1 narrow claim to exact digit |
|
Patient with diabetic neuropathy but no vascular impairment; routine foot care provided |
G0127 (Trim dystrophic nails) |
— (No Q modifier needed) |
RT + T7 (Right foot, 3rd toe) |
E11.40 (Diabetes with neuropathy, unspecified) |
No Q modifier required under neuropathy exception, anatomy still required |
Frequency & Utilization Rules
Even when Q modifiers and anatomy modifiers are applied correctly, frequency can still trip you up. Medicare doesn’t just want to know what you did — they want to know how often.
The Standard Interval
-
For most MACs, routine foot care tied to systemic conditions is covered no more frequently than once every 60 days.
-
This rule applies whether you’re trimming dystrophic nails, debriding, or managing corns and calluses.
Why the 60-Day Benchmark Exists
-
Medicare assumes routine foot care should not require intervention more often unless complications accelerate risk.
-
The 60-day cycle is their benchmark for “reasonable and necessary” utilization.
-
If you bill earlier, you need rock-solid documentation of medical necessity.
Medical Necessity Exceptions
Coverage can be justified at shorter intervals if:
-
Severe vascular compromise leads to rapid nail/callus regrowth that causes pain or ulcer risk.
-
Active diabetic complications make it unsafe for patients to wait 60 days.
-
Documented infections or ulcerations demand more frequent attention.
Provider Note: In these cases, you must clearly explain in your note why a shortened interval is essential. Simply stating “painful nails” won’t cut it.
Jurisdictional Differences
-
Your local LCD (Local Coverage Determination) may have tighter rules — some MACs limit frequency even more strictly or specify the number of visits allowed per year.
-
Always cross-check your LCD annually; rules change and what’s payable in Texas may not fly in New York.
Denial Triggers to Avoid
-
Billing routine foot care every 30–45 days without clear justification.
-
Repeating services at <60-day intervals with vague or templated notes.
-
Failing to tie exceptions to systemic conditions and class findings.
A Quick Step-by-Step Coding Path
When you’re in the weeds of podiatry billing, it helps to think of Q modifiers as part of a simple decision tree. Here’s the cleanest path to follow:
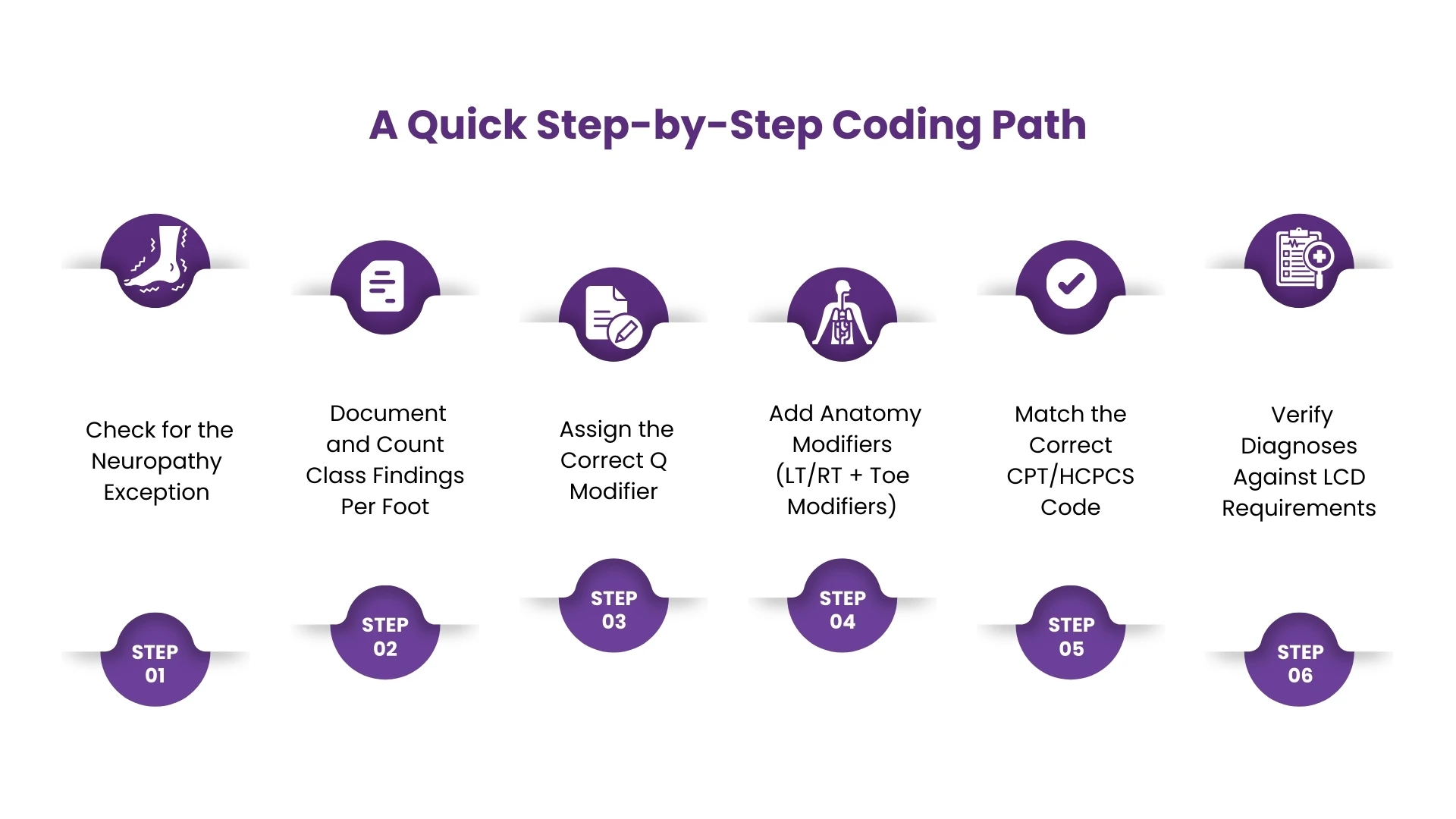
Step 1. Check for the Neuropathy Exception
-
If the patient has peripheral neuropathy without vascular impairment, you do not need Q7, Q8, or Q9.
-
Document the neuropathy clearly and ensure it matches your MAC’s LCD criteria.
-
Still apply laterality (LT/RT) and toe modifiers when relevant.
Step 2. Document and Count Class Findings Per Foot
-
Start with your exam. Note findings foot by foot, not across both feet.
-
Identify whether you have a Class A, two Class B, or one Class B + two Class C findings.
-
This tells you whether Q7, Q8, or Q9 is appropriate.
Step 3. Assign the Correct Q Modifier
-
Q7 = one Class A
-
Q8 = two Class B
-
Q9 = one Class B + two Class C
-
Remember: findings must all come from the same foot.
Step 4. Add Anatomy Modifiers (LT/RT + Toe Modifiers)
-
Always specify which foot (LT = left, RT = right).
-
If a specific toe is treated, add the correct T modifier (TA–T9).
-
Example: 11720 + Q9 + LT + T1 = debridement of one to five nails, left second toe, with documented Q9 criteria.
Step 5. Match the Correct CPT/HCPCS Code
Use the appropriate service code based on the procedure performed:
-
11055–11057 (Corns/calluses)
-
11719 (Trim nails)
-
G0127 (Trim dystrophic nails)
-
11720–11721 (Debridement of nails)
Step 6. Verify Diagnoses Against LCD Requirements
-
Always check your MAC’s LCD and Billing Article for required primary and secondary diagnoses.
-
Some diagnoses are only payable if paired with systemic conditions like diabetes or vascular disease.
-
Watch for asterisked diagnoses that demand proof of active physician care within the last six months
Closing Thoughts
Q7, Q8, and Q9 may look like tiny modifiers, but they carry the weight of compliance, medical necessity, and revenue protection in podiatry billing. Misapply them, and your claims stall in denials. Use them correctly, and you safeguard your reimbursements, prove necessity with confidence, and keep your practice audit-ready.
The truth is, most denials don’t happen because providers lack clinical skill, they happen because billing rules weren’t translated properly into claims language. That’s where a specialized billing partner makes all the difference.
At HMS USA LLC, we take the burden off your shoulders by handling Q modifiers, LCD compliance, and all the details that slow practices down. With HMS USA LLC’s podiatry billing services, you get a partner who protects your revenue by coding correctly, applying modifiers properly, and ensuring claims meet every compliance standard. The result: fewer denials, faster payments, stronger cash flow.
ABOUT AUTHOR

Danial Garcia
As a blog writer with years of experience in the healthcare industry, I have got what it takes to write well-researched content that adds value for the audience. I am a curious individual by nature, driven by passion and I translate that into my writings. I aspire to be among the leading content writers in the world.