Did you know neck pain is a global health burden, affecting millions each year? Studies suggest upwards of 70% of the population will experience neck pain at some point in their lives. As a healthcare provider, you're likely well-versed in diagnosing and treating this prevalent condition. But ensuring accurate reimbursement for neck pain treatment hinges on another crucial step: proper ICD-10 coding.
Confused by the ever-evolving world of ICD-10 codes for neck pain? Fear not! This guide is designed to unravel the complexities and empower you, the healthcare provider, to navigate neck pain coding with confidence. We'll delve into the specific ICD-10 categories, explore best practices for selecting the right code, and shed light on common pitfalls to avoid. By the end, you'll be equipped to ensure your coding reflects the nuanced realities of neck pain, optimizing patient care and maximizing reimbursement efficiency.
What ICD-10 Code Should Be Used to Bill Neck Pain?
The most commonly billable code for neck pain without a readily identifiable cause is M54.2, also known as cervicalgia. Healthcare providers need to report the same ICD-10 code for neck pain.
Many providers encounter cases where patients report pain on one side of the neck, which prompts providers to determine the appropriate scenario to report. While there aren't separate codes for laterality (left-sided vs. right-sided), providers must accurately document the patient's symptoms and use the appropriate coding guidelines.
Categories of Neck Pain & Their Related ICD 10 Codes
Neck pain can stem from numerous causes, each with its associated code that enables healthcare providers to specify the type of pain and its origin. Below are the primary categories of neck pain, alongside their relevant ICD-10 codes, to guide you in selecting the most appropriate one for billing purposes.
Cervical Disk Disorder
This category encompasses various disc-related issues in the neck. The billable icd 10 code is M50.
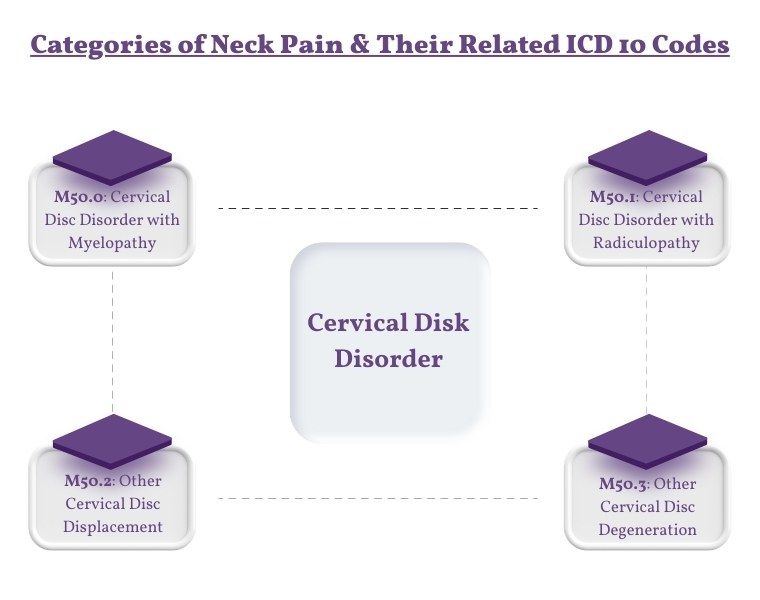
M50.0: Cervical Disc Disorder with Myelopathy
This code is used for conditions where disc disorders lead to myelopathy, a pathology that affects the spinal cord within the cervical region. Patients may present with symptoms such as neck pain, weakness, numbness, or difficulty in coordination, often extending beyond the neck to affect arms or legs.
Coding Tips: Documentation should include the presence of myelopathy signs and symptoms and any radiographic evidence supporting the diagnosis. Detailing the level of the cervical spine affected can enhance coding accuracy and facilitate targeted treatment approaches.
M50.1: Cervical Disc Disorder with Radiculopathy
This code addresses cervical disc disorders that result in radiculopathy, characterized by pain and neurological symptoms that radiate along the nerve pathway. This can include sharp pain, tingling, or weakness in the arms or shoulders resulting from nerve root compression.
Coding Tips: It's essential to document the specific nerve roots involved and the nature of neurological deficits observed. Including diagnostic test results, such as MRI or nerve conduction studies, can substantiate the presence of radiculopathy for coding and treatment purposes.
M50.2: Other Cervical Disc Displacement
This code is used for instances of cervical disc displacement not classified elsewhere. It encompasses scenarios where a disc has moved from its normal position, potentially causing pressure on spinal nerves or the spinal cord without definitive myelopathy or radiculopathy.
Coding Tips: Specify the location of the displacement and any associated symptoms, even if they do not strictly meet the criteria for myelopathy or radiculopathy. Imaging findings that confirm displacement should be included in the patient's record.
M50.3: Other Cervical Disc Degeneration
This code is for degenerative conditions of the cervical discs not captured by more specific codes. Degeneration can lead to neck pain and stiffness, with varying degrees of symptom severity.
Coding Tips: Detailing the degree of degeneration observed and its impact on the patient's functionality can aid in choosing the correct code. Include any relevant imaging studies or physical examination findings that highlight the degenerative changes.
Cervical Spondylosis (M47)
Cervical spondylosis, classified under the broader category M47 in the ICD-10, is a condition characterized by degeneration of the cervical spine, including the vertebrae, intervertebral discs, and joints.
Specific ICD-10 Codes for Spondylosis
M47.2 - Other Spondylosis with Radiculopathy: This code is used for spondylosis that causes radiculopathy, a condition where nerve roots are irritated or compressed, leading to neurological symptoms such as pain, numbness, tingling, or weakness in the limbs. Radiculopathy can occur in various regions of the spine but is coded under specific categories based on its location.
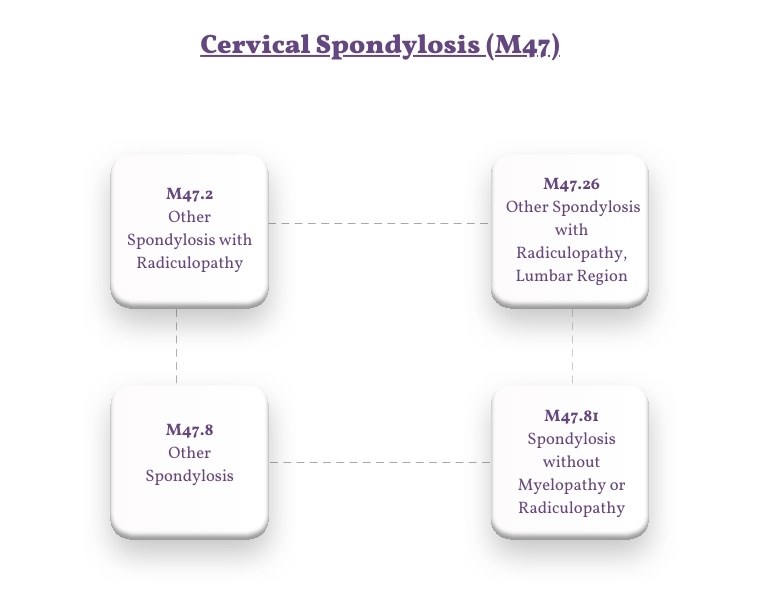
M47.26 - Other Spondylosis with Radiculopathy, Lumbar Region: This specific code addresses spondylosis in the lumbar region that results in radiculopathy, highlighting the importance of specifying the affected spinal segment for accurate diagnosis and treatment planning.
M47.8 - Other Spondylosis: This category encompasses forms of spondylosis not otherwise classified under more specific codes. It covers a range of spondylosis conditions without specifying the presence of myelopathy or radiculopathy.
M47.81 - Spondylosis without Myelopathy or Radiculopathy: This code is designated for cases of spondylosis where neither spinal cord compression (myelopathy) nor nerve root compression (radiculopathy) is present. It's used for spondylosis characterized primarily by pain and stiffness without the neurological complications seen in other variants.
Clinical Application and Documentation
When documenting and coding for spondylosis and its variations, healthcare providers should:
-
Specify the Affected Region: Clearly identifying the spinal region affected by spondylosis is crucial for accurate coding, particularly because treatment approaches can vary significantly based on the location of the degeneration and symptoms.
-
Detail the Presence of Complications: Indicate whether the patient is experiencing complications such as myelopathy or radiculopathy, as these conditions significantly impact treatment options and patient prognosis.
-
Record Comprehensive Treatment Plans: Documentation should reflect the comprehensive management strategy, including conservative measures, interventional pain management techniques, and surgical interventions if applicable. This ensures that the coding accurately reflects the complexity and specificity of the care provided.
Whiplash Injury (S13.4)
Whiplash injuries are acute neck injuries resulting from a rapid, forceful back-and-forth movement of the neck, akin to the cracking of a whip. The ICD-10 classification for whiplash injuries under the code S13.4 highlights the need for specificity in diagnosing and documenting this condition.
Best Practices for Coding Neck Pain
When it comes to ICD-10 coding for neck pain, adhering to best practices not only ensures compliance and accurate billing but also contributes to high-quality patient care. By refining your approach to documentation and coding, you can minimize errors, streamline the billing process, and enhance patient outcomes. Here’s an expanded look at the best practices and common pitfalls in coding neck pain.
1. Comprehensive Documentation
Clearly document the onset, duration, intensity, and character of the neck pain. Note any aggravating or relieving factors. Where possible, identify and record the underlying cause of the neck pain, whether it's an injury, degenerative disease, or another condition. Describe the exact location of the pain. If the pain radiates, specify the pathway and extent.
2. Regular Review of Guidelines
Coding guidelines and the ICD-10 code set are updated regularly. Stay informed of these changes through official channels like the WHO or your local health authority. Training and Education: Participate in continuous education opportunities and training sessions on ICD-10 coding to ensure your knowledge remains current.
3. Utilizing Specific Codes
Aim for the highest level of specificity when selecting an ICD-10 code. This might involve using additional codes to capture the patient's condition thoroughly. Include codes for any related conditions or comorbidities that may influence the treatment of neck pain, ensuring a comprehensive patient profile.
Final Words
Mastering ICD-10 coding for neck pain is essential for healthcare providers, not just for ensuring accurate billing and reimbursement but also for enhancing patient care. By adopting best practices such as detailed documentation, regular review of coding guidelines, and the use of specific codes, providers can avoid common pitfalls like overusing general codes or inaccurately documenting laterality.
This diligent approach to coding not only streamlines the administrative process but also contributes significantly to the quality of patient management and treatment. As the medical field continues to evolve, staying informed and proficient in coding practices will remain a cornerstone of effective healthcare delivery.
ABOUT AUTHOR

John Wick
As a blog writer with years of experience in the healthcare industry, I have got what it takes to write well-researched content that adds value for the audience. I am a curious individual by nature, driven by passion and I translate that into my writings. I aspire to be among the leading content writers in the world.