Every condition in the ICD-10 classification system carries a story, and hypogonadism is no exception. Hypogonadism, defined by the reduced production of sex hormones such as testosterone or estrogen, presents unique challenges in medical coding.
Its causes range from primary gonadal issues to secondary dysfunctions involving the hypothalamic-pituitary-gonadal axis. Capturing these complexities in ICD-10 codes requires a thorough understanding of clinical presentations.
This guide focuses on decoding the most frequently used ICD-10 codes for hypogonadism, such as E29.1 (testicular hypofunction) and E23.0 (hypopituitarism). By understanding these codes, coders can ensure that medical records accurately represent the disorder.
Different Types of Hypogonadism and Their ICD-10 Codes
Hypogonadism is broadly categorized into two types: Primary Hypogonadism and Secondary (Central) Hypogonadism. Each type has distinct causes, pathophysiology, and ICD-10 codes, reflecting the underlying mechanism of the condition.
ICD-10 Codes for Primary Hypogonadism
E29.1 – Testicular hypofunction (for males):
-
This code applies to conditions like testosterone deficiency due to testicular failure, Klinefelter syndrome, or other testicular dysfunctions.
-
It also includes cases such as orchitis, testicular trauma, or chemotherapy-induced testicular damage.
E28.39 – Other primary ovarian failure (for females):
-
Used for ovarian dysfunction conditions such as premature ovarian failure or resistant ovary syndrome.
-
It covers cases where estrogen production is insufficient due to intrinsic ovarian defects.
ICD-10 Codes for Secondary Hypogonadism
E23.0 – Hypopituitarism:
-
This code covers hypogonadotropic hypogonadism caused by pituitary gland dysfunction, such as pituitary adenomas, pituitary apoplexy, or Sheehan’s syndrome.
-
It also applies to panhypopituitarism, where multiple pituitary hormones are deficient.
E23.1 – Drug-induced hypopituitarism:
-
Used when hypogonadism arises from medications affecting pituitary function, such as prolonged use of glucocorticoids.
E23.2 – Diabetes insipidus of pituitary origin:
-
While not always a direct cause of hypogonadism, this condition may co-exist with pituitary dysfunction leading to central hypogonadism.
E23.3 – Hypothalamic dysfunction:
-
This code applies to cases of hypothalamic disorders impacting the release of gonadotropin-releasing hormone (GnRH), causing secondary hypogonadism.
Key Differences Between Primary and Secondary Hypogonadism
|
Aspect |
Primary Hypogonadism |
Secondary Hypogonadism |
|
Origin |
Gonadal failure (testes/ovaries) |
Hypothalamus or pituitary dysfunction |
|
Gonadotropin Levels |
High (LH and FSH) |
Low or normal (LH and FSH) |
|
Common Causes |
Genetic syndromes, trauma, infection |
Pituitary tumors, hypothalamic disorders |
|
Key ICD-10 Codes |
E29.1, E28.39, E89.5 |
E23.0, E23.1, E23.3 |
When Hypogonadism is Unspecified
In some cases, hypogonadism may be diagnosed without sufficient detail to determine its type (primary or secondary) or specific cause. These instances are classified as unspecified hypogonadism in ICD-10 coding. This occurs when the available clinical information or diagnostic workup does not allow for further categorization, but the condition is clearly present.
ICD-10 Codes for Unspecified Hypogonadism
-
E29.9 – Testicular dysfunction, unspecified (for males):
This code is used when a male patient exhibits symptoms of hypogonadism (such as low testosterone levels, reduced libido, infertility, or decreased muscle mass), but the underlying cause (testicular, pituitary, or hypothalamic) has not been identified.
2. E28.9 – Ovarian dysfunction, unspecified (for females):
Applied in cases where a female patient presents with hypogonadal symptoms (such as irregular menstruation, infertility, or low estrogen levels), but the specific cause, whether ovarian or secondary, remains unclear.
ICD 10 Code for Hypogonadotropic Hypogonadism
Hypogonadotropic hypogonadism, in certain cases, falls under the ICD-10 code G11.5, as per AAPC. This code is specifically assigned to the condition when it is part of a broader syndrome, such as 4H syndrome (Hypomyelination, Hypogonadotropic Hypogonadism, and Hypodontia). This rare genetic disorder presents a triad of symptoms, including:
When to Use G11.5
-
G11.5 is applicable in cases where the hypogonadotropic hypogonadism is a part of this specific genetic condition.
-
It is crucial to document the presence of hypomyelination and/or hypodontia to accurately justify the use of G11.5.
ICD-10 Codes for Personal History of Hypogonadism
-
For Male Patients:
Z87.438 – Personal history of other diseases of the male genital organs
This code is specifically used to document a past medical condition affecting the male genital organs, such as hypogonadism, that is no longer active but may necessitate continued monitoring or follow-up care.
It reflects conditions that have implications for future care, such as infertility or the risk of relapse in hormone deficiency.
2. For Female Patients:
Z87.42 – Personal history of other diseases of the female genital tract
This code applies to females who have had a resolved condition, like ovarian dysfunction or estrogen deficiency due to hypogonadism, that requires documentation for future monitoring or management.
It ensures that the patient’s reproductive health history is properly recorded, particularly if it impacts current or future treatment plans.
When to Use Personal History Codes
These codes are used in scenarios where hypogonadism is no longer an active condition but remains relevant to the patient’s overall health record. Examples include:
-
Monitoring for Relapse or Long-Term Effects:
A patient with a history of hypogonadism may still require periodic hormone testing or monitoring for complications like osteoporosis or infertility. -
Risk Assessment for Future Conditions:
Documentation of prior hypogonadism is critical if it predisposes the patient to associated health risks, such as cardiovascular disease or metabolic syndrome. -
Management of Residual Symptoms or Sequelae:
Even after resolution, some patients may exhibit lingering effects that need ongoing observation, such as delayed secondary sexual development.
Coding Guidelines
-
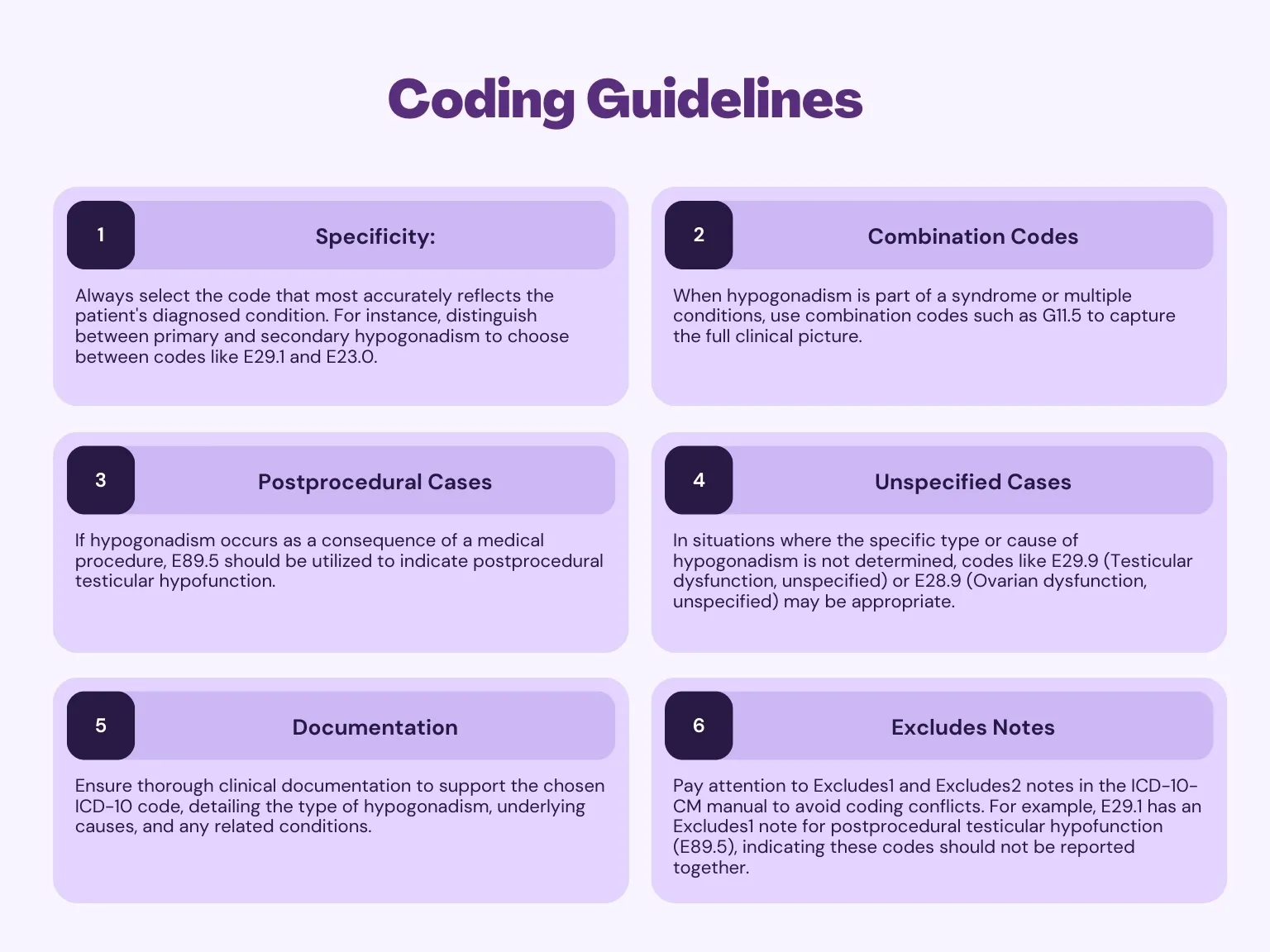
Specificity: Always select the code that most accurately reflects the patient's diagnosed condition. For instance, distinguish between primary and secondary hypogonadism to choose between codes like E29.1 and E23.0.
-
Combination Codes: When hypogonadism is part of a syndrome or multiple conditions, use combination codes such as G11.5 to capture the full clinical picture.
-
Postprocedural Cases: If hypogonadism occurs as a consequence of a medical procedure, E89.5 should be utilized to indicate postprocedural testicular hypofunction.
-
Unspecified Cases: In situations where the specific type or cause of hypogonadism is not determined, codes like E29.9 (Testicular dysfunction, unspecified) or E28.9 (Ovarian dysfunction, unspecified) may be appropriate.
-
Documentation: Ensure thorough clinical documentation to support the chosen ICD-10 code, detailing the type of hypogonadism, underlying causes, and any related conditions.
-
Excludes Notes: Pay attention to Excludes1 and Excludes2 notes in the ICD-10-CM manual to avoid coding conflicts. For example, E29.1 has an Excludes1 note for postprocedural testicular hypofunction (E89.5), indicating these codes should not be reported together.
ABOUT AUTHOR

Pedro Collins
As a blog writer with years of experience in the healthcare industry, I have got what it takes to write well-researched content that adds value for the audience. I am a curious individual by nature, driven by passion and I translate that into my writings. I aspire to be among the leading content writers in the world.