Most billing teams know POS 32 exists. Few really understand when it applies, and even fewer verify it before submitting. That gap is where claims die.
If you're billing for physician services in a nursing facility, POS 32 in medical billing is one of the highest-risk codes you'll touch in 2026. CMS is actively tracking it. The OIG flagged it. And enforcement through CR 13767 (effective July 2025) means there's no more guessing your way through it.
This guide covers everything: the POS 32 description, when to use it, what guidelines apply, how it differs from POS 31, and the mistakes that are costing providers real money right now.
What Is POS 32?
POS 32 stands for Nursing Facility. Per the CMS Place of Service code set, it applies to:
"A facility which primarily provides to residents skilled nursing care and related services for the rehabilitation of injured, disabled, or sick persons, or, on a regular basis, health-related care services above the level of custodial care to other than individuals with intellectual disabilities."
Put simply: POS 32 is for long-term care residents who are NOT under a Medicare Part A skilled nursing facility stay.
That one sentence is where 90% of the confusion lives.
Is POS 32 Inpatient or Outpatient?
This question comes up constantly. The answer matters because it affects your reimbursement rate.
POS 32 is classified as a facility setting. That means Medicare reimburses physician services at the facility rate (lower than the non-facility/office rate). The facility bills separately for overhead and room costs. The physician component is adjusted down accordingly.
So no, POS 32 is not outpatient in the traditional sense. And it's not inpatient the way a hospital admission (POS 21) is. It occupies its own billing category specific to long-term care nursing facilities.
For providers who do a lot of nursing home rounding, this rate distinction adds up. Billing POS 32 when POS 11 (office) might seem easier is not just a compliance problem. It's the kind of pattern that draws a RAC audit.
Our team at HMS handles nursing home billing daily. If you want a quick look at how these facility-rate distinctions affect your practice, our nursing home billing services breaks it down:
POS 32 vs POS 31: What's the Difference?
This is the question that causes the most denials. And it's not because billers don't know the definitions. It's because the same physical building can require both codes, depending on the patient's status that day.
Here's the breakdown:
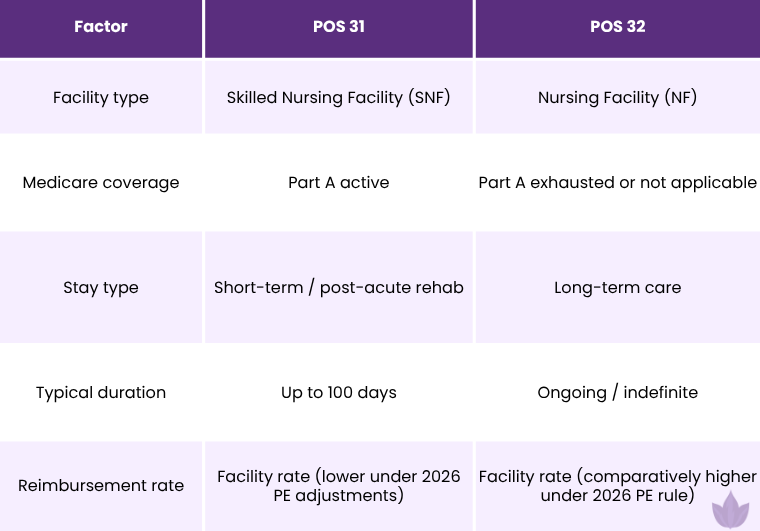
The 2026 Medicare Physician Fee Schedule Final Rule made this distinction more financially significant than ever. CMS' new practice expense methodology reduced indirect PE values for SNF services (POS 31) while comparatively increasing them for NF services (POS 32). The gap in reimbursement between the two codes is wider in 2026 than it was even a year ago.
That means incorrectly billing POS 32 when the patient is under Part A could look like intentional upcoding. CMS is watching this pattern closely.
For a full breakdown of POS 31 rules, read our complete guide
When to Use POS 32
Use POS 32 when a physician or qualified provider renders services to a patient who:
-
Resides in a nursing facility long-term (not under a qualifying hospital stay)
-
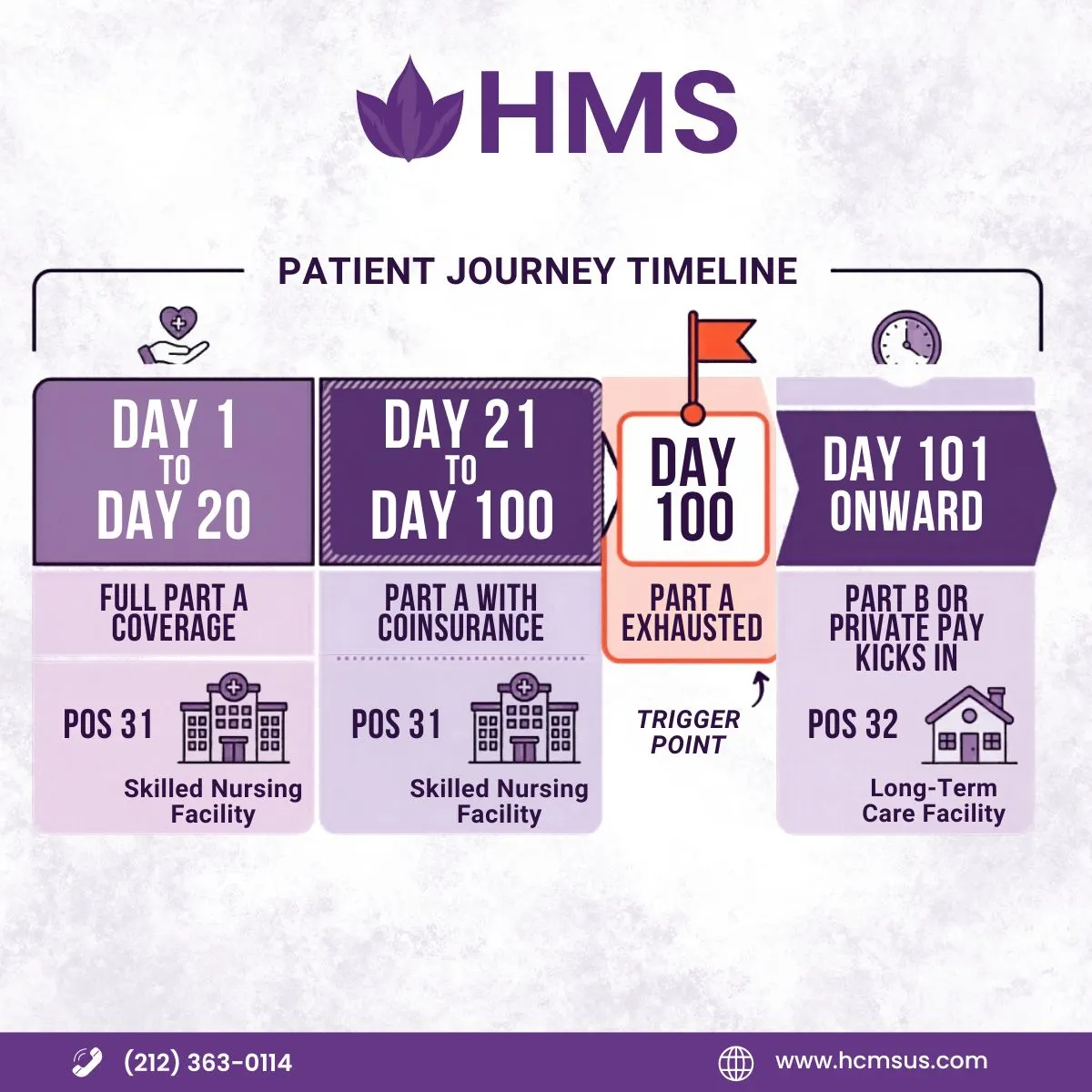
Has exhausted their Medicare Part A SNF benefit (typically after day 100)
-
Was never eligible for a Part A covered SNF stay
-
Is receiving custodial or maintenance-level care under Medicare Part B or commercial insurance
-
Has transitioned from a Part A stay (POS 31) to long-term status in the same facility
Common clinical scenarios where POS 32 applies:
-
Annual wellness visits for a long-term nursing home resident
-
Chronic disease management (diabetes, CHF, COPD) for a Part B resident
-
Wound care visits for a resident not under a Part A stay
-
Medication management and review
-
Post-day-100 visits for patients who started under Part A but remain in the facility
One scenario providers often get wrong: a patient starts as a Part A SNF resident (POS 31) and, after day 100, the Part A benefit exhausts. They stay in the same room, same facility. The billing code must flip to POS 32. Same building. Same patient. Different code.
If your billing team doesn't have a system to track that transition, denials are automatic.
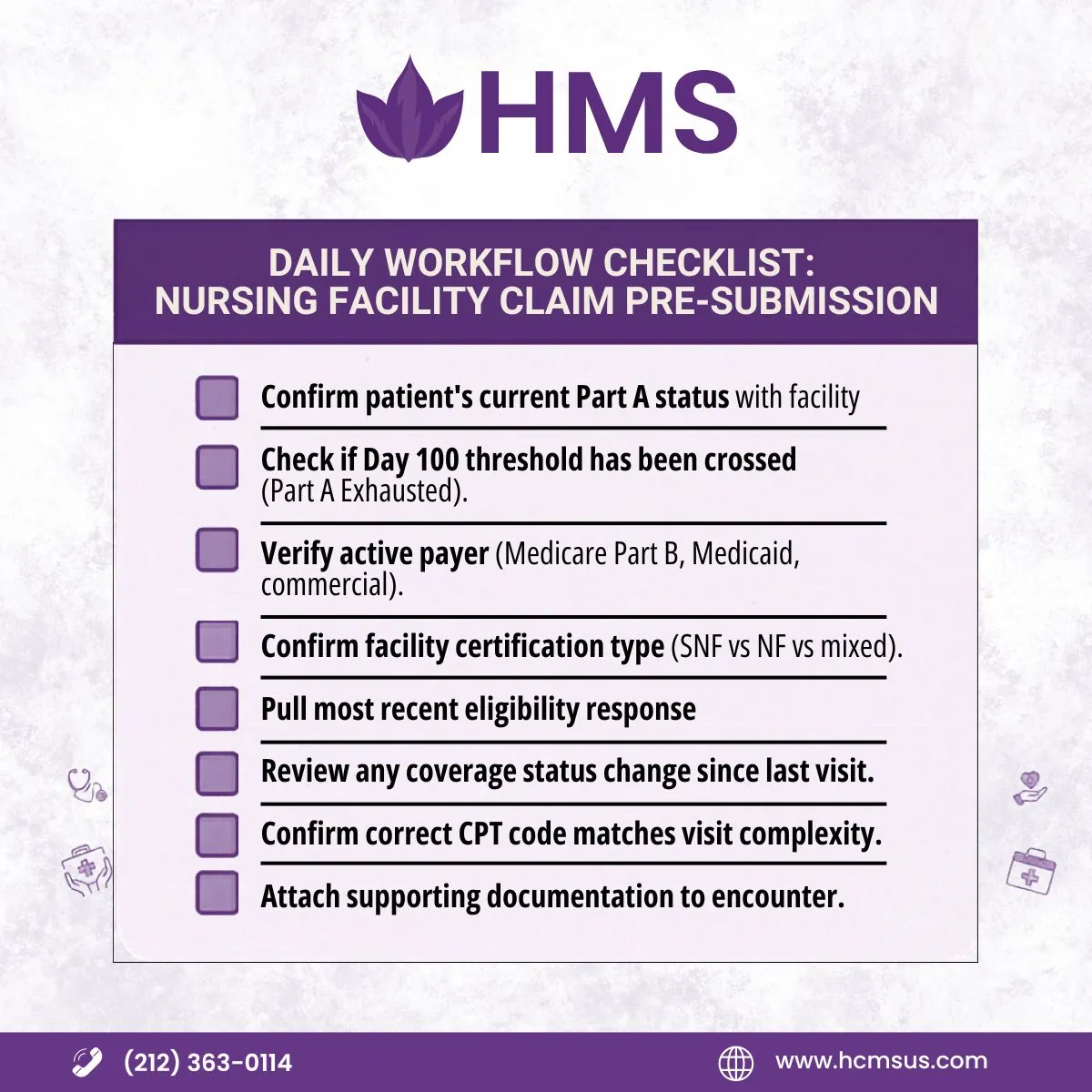
How to Bill for Nursing Facility Services with POS 32
Step-by-step claim submission for POS 32:
-
Verify the patient's current coverage status before every visit. Confirm with facility staff whether the patient is under Part A or Part B.
-
Document the encounter completely. Include the date of service, nature of visit, medical necessity, and any care plan updates. Thin documentation is the second most common reason POS 32 claims get denied.
-
Use the CMS-1500 claim form (or electronic equivalent). Enter POS 32 in Box 24B.
-
Select the appropriate CPT code. For nursing facility E/M visits, you'll typically use 99304-99306 (initial visits) or 99307-99310 (subsequent visits).
-
Match your diagnosis codes. ICD-10 codes must support medical necessity for the visit. Chronic care codes like E11.9 (Type 2 diabetes), I50.9 (heart failure), or N39.0 (UTI) are common.
-
Submit to the correct payer. Medicare Part B processes POS 32 claims for eligible beneficiaries. Medicaid and commercial payers have their own rules, so verify before submitting.
Track remittance carefully. POS 32 has a specific reimbursement rate. Underpayments are worth appealing, especially given the 2026 PE adjustments favoring NF over SNF.
If your practice hasn't had a recent audit of how your nursing facility claims are being submitted, our medical billing audit services can identify gaps before CMS does:
POS 32 Claim Billing Rules: What CMS Requires
The formal rules per CMS, updated through 2025 enforcement (CR 13767):
-
POS 32 must appear on every physician claim for services rendered in a nursing facility where the patient is not under a Part A covered stay.
-
Mixed facilities (those housing both SNF and NF patients) require the billing team to confirm the individual patient's Part A status. The building status doesn't determine the code. The patient's coverage status does.
-
If Part A status cannot be verified, default to POS 31 per CMS guidance. But this is a temporary workaround, not a strategy.
-
Commercial payers may follow Medicare's POS definitions or have their own. Always check payer-specific policies before submitting.
-
For Medicaid, POS rules vary by state. Some states accept POS 32 for Medicaid NF residents; others use different coding structures. Verify with your state's Medicaid MAC.
Does POS 32 Require Modifiers?
This creates real confusion because there is a Modifier 32. They're completely different things.
POS 32 is a place of service code. It goes in Box 24B of the CMS-1500 and identifies where the service was delivered.
Modifier 32 is a procedure modifier. It indicates a mandated service (required by a payer, government agency, or employer). It has nothing to do with nursing facilities.
Pairing Modifier 32 with POS 32 on a claim is not automatically wrong, but it would mean the service was both delivered in a nursing facility AND was a mandated service. That's uncommon. Confusing the two causes immediate claim rejection.
As for other modifiers: POS 32 claims don't routinely require specific modifiers. But certain situations may call for them:
-
Modifier 25: If a significant, separately identifiable E/M service is billed on the same day as a procedure
-
Modifier AI: For principal physician of record in some payer contexts
-
Modifier GW: For services unrelated to a terminal condition (hospice patients)
When in doubt, check the payer's specific modifier requirements. Medicare MACs publish local coverage determinations that spell this out.
For practices managing complex modifier combinations across multiple specialties, our broader medical billing services cover this end-to-end:
Common Mistakes in POS 32 Billing
These are the patterns that generate denials, audits, and recoupments in 2026:
Using POS 32 when the patient is still under Part A. This is the single most flagged error. If the patient's Part A benefit is active and you bill POS 32, you've billed at a higher rate than Medicare allows for that setting. CMS has automated edits specifically to catch this. The claim rejects, or worse, it pays and gets recouped in an audit.
Failing to transition from POS 31 to POS 32 after day 100. The patient's coverage status changes. The billing code must change with it. Many practices miss this because no one built a tracking mechanism for the 100-day threshold.
Assuming the facility type determines the code. POS 31 vs POS 32 is about the patient's coverage status, not which building they're in. A single facility can and does house both Part A and Part B residents simultaneously.
Thin documentation. Payers are increasingly asking for clinical documentation to support POS 32 claims. If the chart doesn't show a visit that required a qualified provider's attention (not just a routine welfare check), the claim is vulnerable.
Skipping eligibility verification. Coverage can change. A patient may transition between Part A and Part B status during a facility stay. Running eligibility only at admission is not enough.
Confusing Modifier 32 with POS 32. As described above, these are unrelated. Incorrect pairing triggers immediate denial.
Using a non-facility rate code (POS 11) for nursing facility visits. It pays more in the short term. It triggers audits and demands for recoupment. It's not worth it.
For providers running rehabilitation services in or adjacent to nursing facility settings, POS 32 intersects with rehab billing rules in ways that add another layer of complexity. Our rehab billing specialists work through these crossover scenarios regularly:
POS 32 Billing: A Quick Reference Table
|
Scenario |
Use POS 32? |
|
Long-term care resident, Part B coverage |
Yes |
|
Patient on day 101 in SNF, Part A exhausted |
Yes |
|
Patient on day 50, active Part A stay |
No (use POS 31) |
|
Routine check-up for nursing home resident |
Yes |
|
Wound care visit, NF resident, Part B |
Yes |
|
Patient admitted to SNF from hospital, day 1 |
No (use POS 31) |
|
Custodial care patient, no Part A ever |
Yes |
|
Mixed facility, cannot confirm Part A status |
No (default POS 31 per CMS) |
POS 32 and the 2026 Reimbursement Shift
This is something billing teams need to know heading into the rest of 2026.
The 2026 Medicare Physician Fee Schedule Final Rule changed how practice expense (PE) is calculated for facility-based services. SNF services (POS 31) took a hit. NF services (POS 32) came out comparatively better.
That means POS 32 now generates higher reimbursement than POS 31 for the same CPT code, depending on the PE component. CMS and the OIG are watching this differential closely. It gives some providers a financial incentive to bill POS 32 even when POS 31 is correct.
That's exactly what they're looking for in audits.
The takeaway: bill what's accurate. Know the reimbursement differential. Make sure your documentation is bulletproof either way.
POS 32 at a Glance
-
POS 32 description: Nursing Facility; for long-term care residents not under a Medicare Part A stay
-
Use when: Part A is exhausted, not applicable, or the patient is a long-term NF resident
-
Don't use when: Part A is active (use POS 31 instead)
-
Reimbursement: Facility rate, comparatively favorable under 2026 fee schedule adjustments
-
Claim form: CMS-1500, Box 24B
-
Most common E/M codes: 99307-99310 (subsequent visits), 99304-99306 (initial visits)
-
Biggest risk: Using POS 32 during an active Part A stay
POS 32 billing isn't complicated once you understand that the code follows the patient's coverage status, not the building they're in. But it requires active verification on every visit. The era of guessing is over. CR 13767 made that official in July 2025, and the 2026 fee schedule changes made accuracy even more financially consequential.
If your nursing facility claims are generating denials, or if you're uncertain whether your team is correctly tracking Part A transitions, talk to our billing team. HMS works with nursing home practices and long-term care providers across the country to get POS coding right from submission day one.
ABOUT AUTHOR

Temba Altman
As a blog writer with years of experience in the healthcare industry, I have got what it takes to write well-researched content that adds value for the audience. I am a curious individual by nature, driven by passion and I translate that into my writings. I aspire to be among the leading content writers in the world.